Introduction
Heliox — a premixed blend of helium and oxygen — has been used in respiratory medicine since Alvan Barach's landmark 1935 paper describing its use for asthma and laryngeal obstruction. Nearly 90 years later, the 80/20 blend remains the clinical standard.
The core problem heliox addresses is straightforward: when airways narrow from obstruction, airflow becomes turbulent rather than laminar, and turbulent flow demands far more muscular effort. Patients in respiratory distress can exhaust themselves simply trying to move air through a constricted passage. Heliox — with helium replacing nitrogen as the dominant gas — dramatically lowers gas density, reducing that resistive burden.
It won't cure the underlying obstruction, but it buys critical time for bronchodilators, corticosteroids, or surgical intervention to take effect — which is precisely where heliox earns its place in acute care.
This overview covers how 80/20 heliox works, its primary clinical indications, delivery methods, and the evidence behind its use.
Key Takeaways
- 80/20 heliox = 80% helium, 20% oxygen — the most common clinical blend
- Reduces gas density, converting turbulent airflow to laminar flow
- Primary uses: upper airway obstruction, croup, severe asthma, COPD exacerbations
- Standard oxygen flowmeters read low; multiply by 1.8 for actual delivered flow
- Not effective when FiO₂ above 0.40 is required; does not treat the underlying condition
What Is 80/20 Heliox and Why This Specific Ratio?
The Physics in Plain Terms
Helium has a molecular weight of just 4.0 g/mol. Nitrogen — which makes up roughly 78% of ambient air — weighs 28.0 g/mol. Because airway resistance in turbulent flow scales with gas density, replacing nitrogen with helium dramatically reduces how hard the body must work to move gas through a narrowed airway.
The notation always lists helium first: 80/20 means 80% helium, 20% oxygen by volume. That's also the most common commercial blend, alongside 70/30 and 60/40.
Why 80% Helium Specifically?
The therapeutic benefit depends on keeping the helium fraction high enough. According to AARC guidance, achieving the full density-reduction benefit requires an FiO₂ at or below 0.40 — meaning helium must comprise at least 60% of the mixture. The 80/20 blend sits well above that threshold, keeping gas density as low as any standard clinical blend allows.
The tradeoffs with other blends:
| Blend | Helium % | Oxygen % | When Used |
|---|---|---|---|
| 80/20 | 80% | 20% | Standard therapy; patients with normal SpO₂ |
| 70/30 | 70% | 30% | Mild supplemental O₂ requirement |
| 60/40 | 60% | 40% | Higher O₂ need; near the therapeutic helium floor |
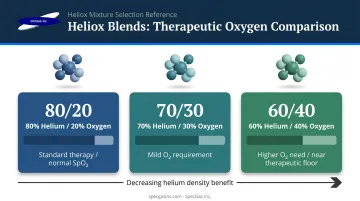
Each step up in oxygen fraction reduces helium and diminishes the density-reduction effect. Patients requiring FiO₂ above 0.40 won't get meaningful therapeutic benefit from any heliox blend.
Heliox doesn't treat airway obstruction — it reduces the physiological burden of breathing through one. Bronchodilators, corticosteroids, or surgery address the root cause; heliox buys time while they take effect.
Clinical Indications for 80/20 Heliox Therapy
Upper Airway Obstruction
This is where heliox has its strongest physiologic rationale. Conditions including laryngeal obstruction, subglottic stenosis, bilateral vocal cord paralysis, post-extubation stridor, and acute vocal cord dysfunction all create fixed upper-airway narrowing. The low density of helium provides immediate resistive relief in these scenarios.
A 2014 critical-care review confirms heliox use as a temporizing measure in post-extubation stridor and tracheal compression. Evidence for inducible laryngeal obstruction and vocal cord dysfunction is limited: a systematic review found only three original studies, all favorable but at high risk of bias.
Croup
Croup is one of the most studied pediatric indications. A 2021 Cochrane review included three RCTs with 91 children aged 6 months to 4 years. Heliox may modestly improve croup scores at 60 minutes in moderate cases, but evidence is low certainty. One comparison of heliox plus saline versus oxygen plus nebulized epinephrine showed little overall difference, suggesting heliox is a useful adjunct rather than a replacement for standard treatments.
Obstructive Lung Disease
The evidence across obstructive lung disease varies by condition:
- Asthma exacerbations: A Cochrane review of 10 RCTs (544 non-intubated patients) found no statistically significant pooled effect on pulmonary function and no reduction in hospital admission rates. Possible benefit was noted in the most severe subgroup, but data were limited.
- COPD: A separate Cochrane review found insufficient evidence to support routine use.
- Carrier gas for bronchodilators: Heliox offers a practical advantage as a delivery vehicle for nebulized albuterol. The low-density mixture improves aerosol deposition in distal airways — a mechanistically sound benefit that standard RCT designs often fail to capture cleanly.

Mechanically Ventilated Patients
When patients with severe obstructive disease require ventilator support, heliox can reduce the flow-resistance burden that makes ventilation difficult. A Respiratory Care study using heliox at 65–70% helium found peak airway pressure dropped from 54.1 to 47.9 cm H₂O and PaCO₂ fell from 64.3 to 62.3 mmHg. Plateau pressure and total PEEP were not significantly changed, meaning heliox addresses resistive and flow-related measures rather than static hyperinflation.
Emerging Applications
These areas have limited or preliminary evidence:
- Congenital diaphragmatic hernia in neonates (one retrospective study, n=28)
- Bronchiolitis: a systematic review found low-quality evidence that heliox does not reduce need for CPAP, intubation, or hospital length of stay
- ARDS and COVID-19: evidence remains preclinical or review-level; no robust clinical trials support efficacy claims
Delivery Methods for 80/20 Heliox
Common Delivery Interfaces
The AARC lists these delivery options for spontaneously breathing patients:
- Non-rebreathing mask (NRB) — most common for acute settings
- High-flow nasal cannula (HFNC) — effective for patients with elevated flow demand
- Standard nasal cannula — suitable for lower-acuity or supplemental use
- Aerosol nebulizer — enables bronchodilator co-delivery alongside heliox
- Non-invasive ventilation (NIV) — used when additional respiratory support is needed
- Invasive mechanical ventilation — requires ventilator-specific calibration (see below)
One requirement applies across all interfaces: gas flow must meet or exceed the patient's inspiratory demand. Any dilution with room air pulls the helium fraction below 60%, negating the therapeutic benefit.
When the patient is on a ventilator, those delivery requirements become more complex — helium's physical properties affect how the machine reads and delivers gas.
Mechanical Ventilation Considerations
Helium alters ventilator readings for flow, volume, and FiO₂. Several ventilators now include dedicated heliox modes — Hamilton Medical's HAMILTON-G5/S1 is one documented example, requiring flow-sensor calibration after each gas change.
Important practice points:
- Avoid single-limb passive exhalation circuit devices (such as V60 and some home ventilators) — higher flow requirements and inconsistent delivered FiHe make these unsuitable, per AARC guidance
- Use caution with volume ventilation at very low tidal volumes — helium's physical properties affect delivered volume accuracy
- Verify compatibility before use — the Drager Evita Infinity V500, for example, explicitly states it should not be operated with helium mixtures; always check manufacturer documentation
Correction Factors and Flow Measurement with 80/20 Heliox
The 1.8 Flowmeter Correction
Standard oxygen flowmeters are calibrated for oxygen, not heliox. When you use an oxygen flowmeter to deliver 80/20 heliox, the displayed reading must be multiplied by 1.8 to determine actual flow to the patient.
Example: a flowmeter indicating 10 L/min is actually delivering 18 L/min of 80/20 heliox.
Both AARC guidance and published Respiratory Care literature confirm this. A dedicated heliox flowmeter eliminates this calculation entirely.
Cylinder Duration Calculation
Use this formula for H or K cylinders:
Duration (min) = Pressure (psig) × Cylinder Factor ÷ Flow (L/min)
For heliox H or K cylinders, the cylinder factor is 2.5 (per AARC).
Worked example:
- Cylinder pressure: 2,000 psig
- Flow rate: 10 L/min (actual, after correction)
- Duration = 2,000 × 2.5 ÷ 10 = 500 minutes
At higher flow rates, duration drops quickly — a cylinder running at 20 L/min actual flow would last roughly 250 minutes under the same pressure.
Peak Flow Meter Inaccuracy
Standard peak flow meters — including the Mini-Wright — are calibrated for air. A CHEST abstract reported that Mini-Wright readings showed an average 8.1% measured reduction while patients breathed 80/20 heliox, even when true airflow had improved.
Clinicians should not rely on standard peak flow meters to assess heliox therapy response. Instead, monitor:
- Respiratory rate
- Accessory muscle use
- SpO₂
- Patient comfort and work of breathing
One practical note on gas composition: if the actual helium-to-oxygen ratio deviates from labeled 80/20, every correction factor calculation becomes inaccurate — potentially leading to under- or over-delivery of oxygen. Sourcing heliox from suppliers who use NIST-traceable gravimetric blending helps ensure labeled concentrations match actual cylinder contents.
Benefits, Limitations, and Clinical Caveats
Key Benefits
- Therapeutic effects often appear within one hour of initiation, per AARC guidelines
- Delivered through NRB mask or HFNC — no procedural risk, no invasive setup
- Reduced work of breathing: directly addresses the physiological burden of turbulent flow
- Bridge therapy value: may delay or avoid intubation in upper airway obstruction cases
- Potentially improves albuterol deposition in distal airways when used as a bronchodilator carrier
These advantages make heliox a practical first-line option for many obstruction scenarios — but its utility has clear boundaries.
Limitations and Contraindications
- FiO₂ ceiling: not appropriate when patients require FiO₂ above 0.40 — beyond that threshold, helium concentration falls below therapeutic levels
- Heliox addresses airflow mechanics only; the underlying obstruction still requires definitive treatment
- Equipment demands: requires dedicated flowmeters or correction calculations, plus appropriate delivery interfaces
- Continuous high-flow use at 15–20+ L/min depletes cylinders quickly — ongoing cost at that rate adds up
- Helium raises sound wave speed in the vocal tract, shifting pitch noticeably upward; briefing patients and families before starting prevents unnecessary alarm
Monitoring Best Practices
- Use an oxygen analyzer to verify delivered FiO₂ — recalibrate against both air and 100% oxygen regularly
- A helium analyzer adds further assurance of mixture accuracy, particularly when using standard flowmeters with correction factors
- Assess clinical response through respiratory rate, SpO₂, and work of breathing — not standard peak flow meters
Frequently Asked Questions
What is heliox therapy used for?
Heliox is used primarily for upper airway obstruction (including croup, post-extubation stridor, and laryngeal obstruction) and as a supportive measure in severe asthma and COPD exacerbations. It functions as a bridge therapy, reducing the work of breathing while definitive treatment addresses the underlying condition.
What does 80/20 heliox mean?
It means the gas mixture contains 80% helium and 20% oxygen by volume. The notation always lists helium first. The high helium fraction maximizes the density-reduction benefit; 20% oxygen approximates room-air concentration for patient safety.
What is the correction factor for 80/20 heliox?
When delivering 80/20 heliox through a standard oxygen flowmeter, multiply the displayed reading by 1.8 to get the actual flow rate. A flowmeter reading 10 L/min is delivering 18 L/min. A dedicated heliox flowmeter eliminates this adjustment.
Can 80/20 heliox be used for patients who need more than 20% oxygen?
Patients requiring supplemental oxygen above ~20% FiO₂ should use 70/30 or 60/40 blends. However, each increase in oxygen fraction reduces helium below 80% and diminishes the therapeutic density-reduction effect. Above FiO₂ 0.40, the helium fraction falls below the ~60% threshold needed for meaningful benefit.
How long will a heliox cylinder last during therapy?
Use the formula: Pressure (psig) × 2.5 ÷ Flow (L/min) = Duration in minutes. A 2,000 psig H cylinder at 10 L/min actual flow lasts approximately 500 minutes. Higher flow rates reduce duration proportionally.
What are the main limitations of heliox therapy?
Heliox does not treat the underlying airway condition, is ineffective when FiO₂ above 0.40 is required, demands specialized equipment and training, and can be costly at sustained high flow rates. Standard peak flow meters also cannot accurately measure lung function during heliox breathing; clinical signs are the reliable monitoring tool.